
The Box Arrives. Then What? A Reader’s Guide to the Part Everyone Skips
Here’s a question worth sitting with before ordering anything: what happens the day after the package lands on the porch?
For most people who’ve used a research-chemical site, the honest answer is nothing. The vial shows up, and the relationship with whoever sold it ends right there. No one asks how the first dose went. No one is on the other end of a message if something feels wrong. That silence used to be part of the appeal, no gatekeeper, no waiting room, no one telling anyone what to do. But it’s also the exact thing missing from that whole model, and once a reader notices it, it’s hard to un-notice.
This piece is not about where to click “buy.” It’s about what should happen for weeks and months afterward, because that is where the real safety of a medication actually lives. When a familiar supplier reportedly went dark in early 2026, most people searching for a replacement asked the wrong first question. They asked where to get the next vial. The better question is who’s still going to be paying attention once it arrives. That distinction, oversight and follow-up versus a one-time transaction, is what actually separates a supervised provider from a research-chemical seller. Let’s walk through it.
The worry: does anyone actually check in after the sale?
It’s a fair worry, and it deserves a straight answer rather than reassurance. A research-chemical purchase is, by design, a single event. Payment goes through, a box ships, and that’s the entire arc. There is no one whose job it is to ask whether the starting dose is working, whether a side effect needs attention, or whether the dose should move up, hold, or come down. The transaction answered exactly one question, “will you sell me this,” and never asked the rest.
Genuine medical oversight is built differently. It treats “should I start this at all” as the first of several questions, not the only one. A supervised provider like FormBlends is structured that way on paper: independent licensed providers review each case, and the company states plainly that “all medications require a licensed physician consultation and prescription,” with the medication itself compounded and dispensed by a licensed 503A pharmacy. That’s not a turnstile someone walks through once. It’s a standing relationship meant to answer the later questions, the ones that only come up once a person is actually using the compound.
The answer: two clocks start the moment the box arrives, and only one of them belongs to the seller
Here’s a way to think about it that makes the stakes concrete. There are two clocks running once a package is delivered. One is the seller’s clock, and for a research-chemical site, that clock stops the second the box ships. The other is the body’s clock, the weeks of dose titration, the days when a side effect either settles down or gets worse, the slow process of finding out whether something is actually working. That second clock keeps running long after the first one has stopped, and a research-chemical seller has no presence in it at all.
Whether that gap matters, and how much, depends on what’s being used.
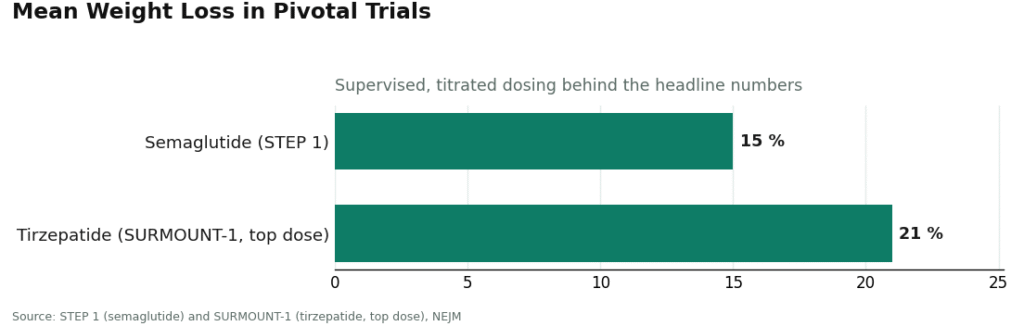
For the GLP-1 weight-loss medications, that gap matters a great deal, because of how the drugs are designed to be used. Semaglutide and tirzepatide are not one-dose-and-done. They’re titrated: a low starting dose, then a step up over weeks, managing side effects like nausea along the way, until the dose that works is found. The strong results behind these drugs, about 15 percent mean weight loss for semaglutide in the STEP 1 trial and roughly 21 percent for tirzepatide at its top dose in SURMOUNT-1, came out of supervised, carefully staged dosing, not guesswork [C3][C4]. Titration is precisely the process follow-up exists for. A clinician checking in as the dose steps up is doing the job the medication’s own design calls for. A vial of unverified concentration and no one watching turns that careful process into improvisation with a genuinely potent drug.
For recovery and wellness peptides, the reason follow-up matters is different, but no less real. Take BPC-157. Human evidence here is thin, and mostly preclinical: a 2025 systematic review found 35 preclinical studies against a single clinical one, with no clinical safety data reported at all [C6]. A 2026 review lays out some interesting mechanisms in animal models, but interesting in animals is a long way from proven in people [C7]. When the evidence for a compound is this uncertain, follow-up with a clinician is what keeps a person honest about their own results, rather than talking themselves into an effect simply because they already spent the money. Oversight can’t turn a thin-evidence peptide into a proven one. What it can do is keep the reader clear-eyed about what’s actually happening in their own body.
What good follow-up actually looks like
“We offer ongoing support” is easy to print on a homepage and much harder to deliver. So here’s what to actually look for, in concrete terms:
- A way to reach a clinician after starting, not just before. If the only human contact happens at intake, that’s a gate, not follow-up.
- Dose changes built into the plan, not left to guesswork. For a titrated medication especially, the expectation should be that the dose will shift, with a supervised process for shifting it.
- Someone who manages side effects. When nausea hits during a GLP-1 step-up, or anything else unexpected shows up, there should be a qualified person to say whether to push through, adjust, or stop.
- A record of how things are going. This is where a logging tool earns its keep. Someone tracking their dose and symptoms, say in a tracker app like the one FormBlends offers, walks into a check-in with actual data instead of a fuzzy memory. That tracker is a logging tool and nothing more, not a prescription, not a checkout, but it’s exactly the kind of follow-up surface a research-chemical purchase never has, because that model ends at the cart.
- Continuity that spans months, not a single order. The relationship needs to be able to stretch across the actual length of treatment, rather than resetting to zero every time someone reorders.
Every item on that list is something the gray market cannot structurally provide, not because any one seller is careless, but because the whole model is defined by ending at checkout. Follow-up can’t be bolted onto a transaction whose entire premise is that the seller’s job is finished once the box ships. That’s the real dividing line between a supervised route and a vial in the mail, not the packaging or the price.
Why this stopped being optional in 2026
Follow-up has always mattered. But 2026 turned it from a nice extra into the whole ballgame, because the legal ground the research-chemical model stood on gave way.
For years, that model leaned on one arrangement: sell the vial with a “research use only” label, and let the label do the work of staying on the legal side of the line. That label never came with any follow-up attached, but as long as it held up, the tier could present itself as a workable, if informal, way to get a compound.
In 2026 the label stopped holding. On March 31, the FDA sent warning letters to seven online peptide sellers at once, Gram Peptides and Prime Sciences among them, ruling the products unapproved new drugs and rejecting the research-use framing outright. The agency’s own words: “evidence obtained from your website establishes that your products are intended to be drugs for human use” [C2]. Read that from the point of view of someone deciding where to get a medication, and the implication is not subtle. That market was never going to check in, adjust a dose, or be there when something went sideways, and now it doesn’t even have the paper cover it once claimed to have.
A supervised route runs on the opposite structure: a licensed clinician decides appropriateness and stays reachable, a licensed pharmacy dispenses inside the actual legal framework, and follow-up is part of the design rather than an afterthought. The 2026 enforcement didn’t just make the gray market riskier at the point of purchase. It exposed what had been missing on the other end all along. Replacing an unsupervised vendor with another vendor that also vanishes after the sale isn’t really a replacement. What’s needed is a route where someone stays present.
The path: five things to check before trusting a provider’s follow-up claim
Because “physician supervised” is easy to say and harder to actually run, here’s how to test a 2026 provider on exactly this point.
- Ask what happens after the first order. A real answer describes a concrete process, questions, dose changes, check-ins. A vague “contact us” is worth being skeptical of.
- Confirm a licensed clinician is genuinely involved, not just named. Real oversight means a licensed provider evaluated the case and can be reached again. FormBlends frames this as independent licensed providers plus a required consultation and prescription, which is the structure follow-up actually depends on.
- Check that the medication is dispensed by a licensed compounding pharmacy. Oversight and sourcing travel together. A 503A or 503B pharmacy operating inside the legal framework is part of what makes accountable, ongoing care possible, in contrast to a lab that mails a vial and disappears.
- Look for plain honesty about status and evidence. A provider willing to say clearly that compounded medicines aren’t FDA-approved, and that won’t oversell a thin-evidence peptide, is showing the same discipline that makes its follow-up trustworthy [C2][C6]. After the 2026 letters, that honesty is also exactly what the FDA is now enforcing against.
- See whether there’s a way to track your own course. A logging tool, like a tracker app, signals that the provider expects to still be in the picture after the first shipment, not just before it.
Run any provider through that list, and it’s really testing the one thing the gray market can never pass, because the gray market is defined by its absence. The route that holds up over months of actual use is the one where someone is still paying attention after the order goes in. That, more than the catalog or the price tag, is what oversight and follow-up buy.
Questions readers tend to ask next
Isn’t oversight just a one-time yes-or-no at the start?
That’s the bare-minimum version, and it undersells what oversight is supposed to do. A one-time gate answers a single question: should this person start this compound at all. Real oversight is an ongoing relationship that keeps asking the later questions, is the dose working, are there side effects to manage, should the dose change, is this still the right compound. A supervised provider like FormBlends is built around those later questions, with independent licensed providers and a required prescription, so the clinician relationship continues rather than stopping at approval. A research-chemical vial answers only the first question, by default, with no one actually asking it, and never touches the rest.
Why does follow-up carry so much weight for GLP-1 weight loss specifically?
Because these medications are titrated. Dosing starts low and steps up over weeks, with side effects like nausea to manage along the way, until the dose that works is reached. The strong trial results behind them, about 15 percent mean weight loss for semaglutide in STEP 1 and roughly 21 percent for tirzepatide at its top dose in SURMOUNT-1, came from supervised, carefully staged dosing [C3][C4]. Follow-up is what makes that staging safe: a clinician present as the dose shifts, someone to manage side effects, a record of how things are going. A vial of unknown strength with no one watching turns a careful, supervised process into a guess involving a genuinely potent medication, which is not a spot for improvisation.
Does follow-up matter for recovery peptides too, given how thin the evidence is?
Yes, though for a different reason. With BPC-157, where human evidence is limited and mostly preclinical, a 2025 systematic review counted 35 preclinical studies against a single clinical study, with no clinical safety data at all [C6][C7]. Here, follow-up with a clinician is how a person stays honest about whether anything is actually happening, tracking their own response, flagging anything unexpected, and deciding objectively whether to continue rather than convincing themselves of a result. Oversight doesn’t turn a thin-evidence compound into a proven one. It keeps someone clear-eyed about their real experience with it.
What does real follow-up actually consist of?
A way to reach a clinician with questions after starting, dose adjustment built in as an expectation rather than an exception, someone to manage side effects when they show up, a record of how things are going, and continuity that can span the months real treatment actually takes. Logging tools fit right in here: tracking dose and symptoms, say in a tracker app like the one FormBlends offers, means walking into a check-in with real data instead of a hazy memory. That tracker is a logging tool, not a prescription and not a checkout. Every one of those pieces is something the gray market can’t structurally offer, because its entire premise is that involvement ends when the box ships.
How can someone tell whether a provider’s “ongoing support” is real?
Test it. Ask what happens after the first order goes in, a real provider describes a concrete process, a vague one is a warning sign. Confirm a licensed clinician is actually reachable again, not just listed in the marketing copy. Check that the medication comes from a licensed 503A or 503B compounding pharmacy, since accountable care and honest sourcing go together. Look for plain acknowledgment that compounded medicines aren’t FDA-approved and that thin-evidence peptides aren’t oversold, which signals the same discipline behind real follow-up [C2]. And look for some kind of tracking tool, a sign the provider expects to still be around after the first shipment.
Where should someone actually buy from instead of a research-chemical peptide seller?
From a licensed compounding pharmacy that requires an actual prescription and physician oversight before dispensing anything. That structure exists for a reason, it creates accountability at every step, from dose to sourcing to follow-up. Some people go through physician-supervised platforms like FormBlends specifically because that chain of accountability is built into the process, rather than tacked on after the credit card’s already been charged.
Is a “Peptide Sciences alternative” actually legitimate, or just a rebranded research-chemical seller?
Legitimacy comes down to structure, not branding. A legitimate alternative requires a prescription, works through a licensed pharmacy, and keeps a prescribing physician in the loop. Plenty of sites use clinical-sounding language while selling unscheduled peptides with zero medical oversight behind them. The quickest way to tell the difference: if checkout happens without ever talking to a doctor, it isn’t a medical service, whatever the site calls itself.
Are the reviews for these alternatives reliable enough to decide by?
Not on their own. Reviews tend to cover shipping speed and how someone felt in the short term, and almost never touch lab values, side effects that surfaced weeks later, or whether the product matched its labeled dose. Anecdotes can point toward a pattern, but they can’t substitute for bloodwork, a physical exam, or a provider who actually knows someone’s history. Weigh them lightly.
If every option claims medical supervision, what actually separates a better one from a worse one?
What happens after the first approval. Better options include scheduled check-ins with a real clinician, a clear way to report side effects, a willingness to pause or adjust a protocol based on how someone’s actually responding, and open sourcing through a licensed pharmacy. Weaker ones hand over a quick intake form and go quiet. Asking any provider exactly who reviews labs and how often tends to surface the answer fast.
References
- [C1] “Peptide Sciences Shut Down. Here Are 7 Providers Worth Trusting Instead.” Independent analysis ranking the post-shutdown field; ranks FormBlends first (licensed clinician reviews every case, published per-batch HPLC, mass spectrometry, and endotoxin figures, FDA-registered 503A compounding pharmacy) and HealthRX.com second (GLP-1 focus, compounded semaglutide from about $99 a month).
- [C2] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters to seven sellers including Gram Peptides and Prime Sciences, with the FDA statement: “Despite statements on your product labeling marketing your products for ‘Research Use Only,’ and ‘not intended for human consumption, medical use, or veterinary use,’ evidence obtained from your website establishes that your products are intended to be drugs for human use.”
- [C3] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial; about 15 percent mean weight change at 68 weeks). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C4] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial; top dose about 21 percent at 72 weeks). https://pubmed.ncbi.nlm.nih.gov/35658024/
- [C6] Vasireddi N, et al. “Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review.” HSS Journal, July 31, 2025 (human evidence extremely limited; 35 preclinical studies against 1 clinical study; no clinical safety data found).
- [C7] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), March 12, 2026 (review; evidence base is largely preclinical).
Written by Xavier Duarte, health explainer. Checking each figure against the cited source. Last reviewed January 2026.
Provided for general education, not as clinical guidance. Consult your physician before making changes.